Retinoids are the gold standard skincare ingredients. They’re the next essential product after sunscreen, because they can help with so many skin issues, and there’s scientific evidence to back them up.
But there are a lot of options, so it’s tricky to work out which one you should use – and it doesn’t help that there’s so much incorrect info out there. But the right one can make a huge difference to your skin.
Hopefully this guide can help you out! I have a PhD in medicinal chemistry and am a qualified cosmetic chemist, plus I’ve tried thousands of skincare products over the last decade. So seeing all the myths and traps that people fall for when it comes to retinoids physically hurts me.
In this post I’ll break down drug versus cosmetic retinoids, and the differences between drug and cosmetic retinoids – why drugs are a bit overrated, cosmetics are underrated and compounded retinoids, like those you get from telederm companies, are super overrated. I’ll talk about some pointers for working out which one you should use, and along the way I’ll bust some myths and common traps people fall into when it comes to retinoids.
The video version of this is here, keep scrolling for the written version…

What are retinoids?
If you aren’t already familiar with retinoids, they’re skincare ingredients that work like vitamin A. They attach to retinoid receptors in your skin.
Retinoids are like keys which can fit into these receptor “locks”, and trigger an effect… or rather, a whole bunch of effects, which is why retinoids are so great in skincare (and also why they burn your face off, but we’ll get to that in a bit).

If you’re looking at skincare, you probably have some sort of goal in mind – retinoids will probably help you towards that goal:
Acne
Retinoids can stop pores from clogging up and forming microcomedones, which turn into pimples. Technical version: they normalise epidermal turnover, decrease cellular adhesion, increase follicle clearance, and inhibit inflammatory IL-6, TNF-α, IFN-γ etc.
Uneven pigment
This includes melasma, post-inflammatory hyperpigmentation, and sun spots.
Retinoids can reduce excess melanin pigment production, and speed up pigment clearance by increasing the production and shedding of keratinocyte cells in the upper layers of skin (epidermis).
Smoother skin texture
This includes evening out wrinkles, fine lines, shallow scars and pores.
Retinoids increase collagen, a protein in your dermis which makes it like a thicker, firmer mattress. They also normalise elastin, another dermal protein that becomes thick and uneven with sun damage. There’s higher deposition of glycosaminoglycans in the skin, which makes thicker and plumper, and reverses degenerative chances in keratinocyte skin cells.
There’s also evidence that they can help with many other skin conditions, including psoriasis, red stretch marks, and pre-malignant skin cancers.
But not all retinoids work the same, and not all products with the same retinoid ingredient will work the same either.
Drug versus cosmetic retinoids
Some retinoids are drugs, while others are cosmetic ingredients.
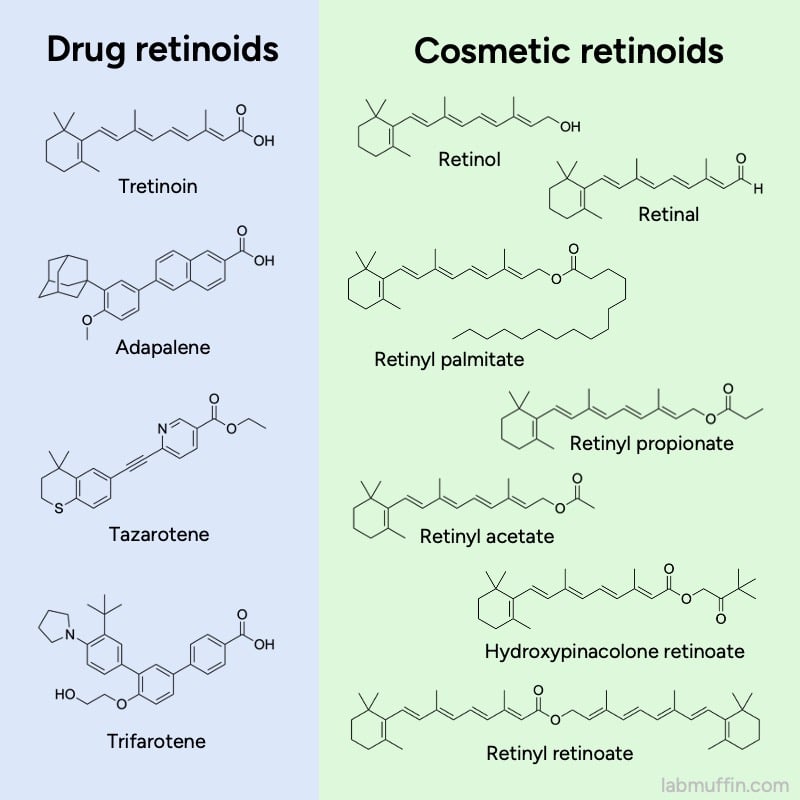
For most of the drugs you’ll need a script from a doctor, although adapalene is available over-the-counter in some places. Cosmetic retinoids like retinol are available in regular skincare products.
There are advantages to both types, but there are a lot of misunderstandings about them, and I think cosmetic retinoids are quite underrated.
Drug retinoid advantages
My PhD was mostly in medicinal chemistry and I studied pharmacology during my undergraduate degree, so when I first started getting into skincare, drug retinoids just seemed obviously better.
Efficacy of ingredient
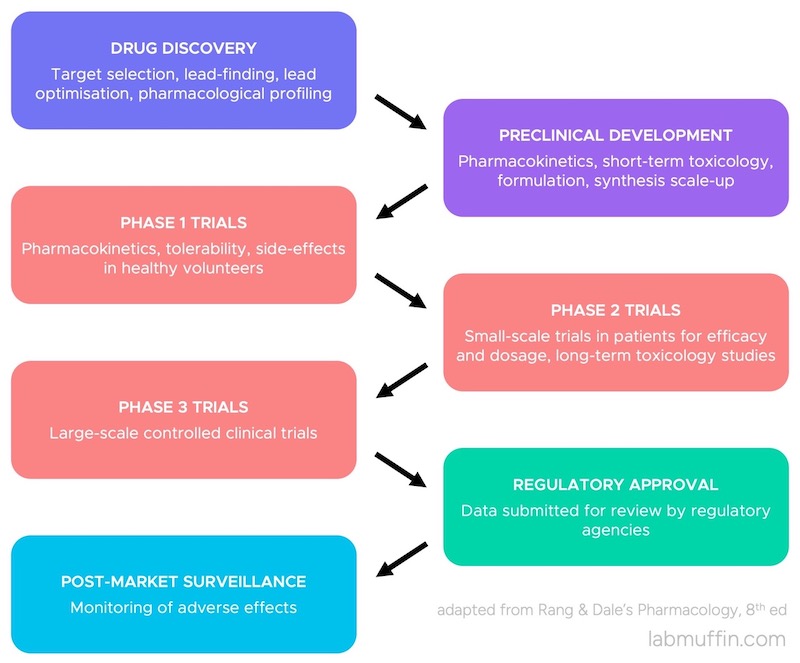
Drug ingredients have demonstrated efficacy. They went through an approval process (like hazing, but for molecules): studies using these were done on lots of people, regulatory agencies with lots of experts checked it, and decided there was enough evidence to show they’re effective.
So when a tube of adapalene says it’ll treat acne, it’s going to do that – or at least the chance of it doing that is much higher (individual factors can affect whether it’ll work for you specifically, but the chances are as good as it gets).
There’s also a lot more independent research on drug ingredients. Scientists from different institutions around the world with no direct financial conflicts of interest will test it, and publish their results. It doesn’t meant that cosmetics don’t work, but there’s more educated guessing required (more details about drug versus cosmetic funding differences in this post.)
Related post: Is Retinol a Scam? The Science
Plus I mean, they gatekeep the stuff – it’s so strong they make you jump through hoops to get it! It just gives off a lot more powerful vibes.
Efficacy of formula
A less obvious but really important upside: drug products are also regulated for the effectiveness of the formula.
Yes, this is partly to do with percentage, but if you’ve read my posts before, you’ll know the overall formula is crucial. You can’t just dump 0.05% tretinoin into a random moisturiser, and expect it to work as well as a regulated formula that’s been optimised.
In short, an effective formula needs to convince the active to leave the applied product layer and go into your skin, deep enough to reach the target – in this case, it’s the retinoid receptors inside your epidermal or dermal cells. Some ingredients go into skin more easily because of their chemical properties, but others need more convincing. For drugs, the formula inside a regulated drug retinoid tube is more or less the same as the one that worked in the scientific studies.
This testing and regulation of drug formulas is where I think one of the biggest myths in skincare comes from, that everyone from standard influencers to medical doctors repeat all the time: the idea that percentage is all-important in cosmetic skincare products.
For drugs, it’s safe to assume that a generic 0.05% tretinoin cream will work pretty similarly to the brand name one… but only because in the background, regulators only approve bioequivalent generic products. Bioequivalent means that not only do they need to just have the same percentage of active, but they need to demonstrate that they work on your body close enough to the already approved drug. (If it doesn’t and they still want to sell it, they’d be required to go through a whole separate approval process.)
How bioequivalence is tested depends on the country and the product. For example, the US FDA recommends doing a 12 week acne clinical trial for tretinoin cream, but for tretinoin gel there’s also the option of doing some (probably cheaper) tests that don’t involve people. The main test involves measuring the rate at which tretinoin diffuses from the gel to a membrane, compared to the already approved version (gels are less variable than creams, so this test gives a pretty good indication).
So most of the time, two drug retinoid products with the same active, percentage and form (e.g. gel, cream) should work pretty much the same – because the ones that didn’t work the same weren’t approved.
But this regulation doesn’t happen with cosmetics. A badly formulated 1% retinol cream might work worse than a well-formulated 0.2% retinol cream that’s actually been optimised to deliver the active to the receptors – but if you only looked at the percentage, you’d end up picking a less effective product.
Stability
Another less obvious upside: drugs are also regulated more for stability.
Both drugs and cosmetics are usually tested for standard stability – for example, it shouldn’t go lumpy, mouldy or irritatingly acidic too fast.
However, with drug retinoids, the stability of the active ingredient in the specific formula and specific packaging has to be guaranteed over time. So if you follow the storage instructions on the tube (which are there for a reason – you should always read them and I totally didn’t read them for the first time when I was preparing for this post!), the concentration should stay reasonably close to the labelled percentage, until the expiry date.

But this isn’t necessarily the case with cosmetics, and it becomes a problem with unstable ingredients like retinoids, which break down faster than most other skincare ingredients.
Now, some cosmetic brands do make the effort to make sure their retinoid product is stable. Neutrogena and RoC are standouts – their jar retinol products last for 12 months after opening. There are also brands who use more stable retinoids, or commercially available stabilised versions.
But the point is, cosmetic brands don’t have to. A brand can legally just dump 1% retinol powder into a random cream and sell it, and it might be mostly broken down by the time it gets to you.
And this isn’t uncommon. One research group tested a bunch of cosmetic retinoids and found that a lot of them decomposed by more than half in the first 6 months after opening. Only 3 out of the 6 retinol products had more than 50% of the original retinol left at the expiry date.
Product quality
Finally, there’s the wider issue of product quality. There’s more of a guarantee that drug products will actually contain what they say they contain.
Both cosmetics and drugs are meant to legally have accurate ingredient lists, but things can slip through the cracks, and mistakes are less likely for drugs.
There’s a set of safeguards for manufacturing products, called Good Manufacturing Practice (GMP). This includes things like:
- making sure ingredients aren’t mixed up
- making sure the ingredient you receive is the one you thought you bought
- checking for impurities
- making sure equipment is clean enough by swabbing and testing it
This is usually done for cosmetics as well, but it’s a lot more variable because it isn’t as regulated (most countries have a licensing system for drug manufacturing facilities, but not cosmetics).
There have been quite a few examples of ingredient mix-ups with cosmetics.
In 2022, The Inkey List got in trouble for somehow putting 3.4% salicylic acid in their 2% salicylic acid cleanser. And while getting more active ingredient seems like a bargain, this didn’t seem intentional given that it’s illegally high (the legal limit is 2% in the EU) – it does make you wonder what else they could be messing up in manufacturing.
The FDA published a study in 2009 where the retinoid concentrations were tested in 29 cosmetic products. 6 of the products (20%) didn’t have the right retinoid, or had a different concentration.
The same retinoid stability researchers mentioned earlier also tested 21 cosmetic products for their actual retinoid content. Almost all of the 7 products with a retinoid percentage on the label had a different amount inside. A lot of these might’ve decomposed, but some of these are higher than the amount on the label. A lot of the products also had a different retinoid inside, which couldn’t be explained by it decomposing.
And again, this can happen with drug products as well, but there are a lot more safeguards against it.
Cosmetic retinoid advantages
So based on all this, drug retinoids should be the obvious choice, right? But the more I tried different products and learned more about cosmetic chemistry, the more I realised it was more complicated than that…
Flexibility in formula
The biggest advantage of cosmetics is that there’s a lot more flexibility in their formulas, which is the flip side of drugs being so strictly regulated.
Once a drug formula is approved, a company can’t really change it much without having to go through a new approval process. This is really expensive, so generally a company won’t release a new formula unless they know enough people will switch to justify the cost.
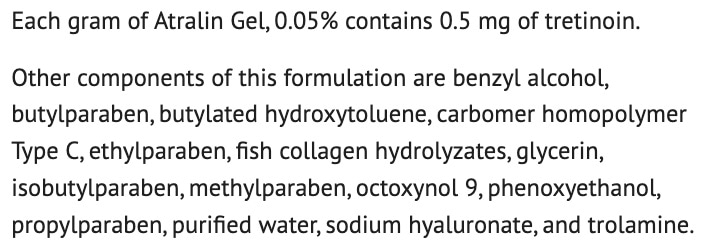
For example, Altreno is 0.05% tretinoin in a lotion base that’s more hydrating and nicer to use, containing hyaluronic acid, collagen and glycerin. The manufacturer was already making 0.05% tretinoin in a gel base, with the same hydrating ingredients (Atralin).

To get the lotion version approved, they needed to submit data including two 12 week Phase 3 trials with a total of 1640 participants. If we take the averages from Sertkaya et al (2016) as a very rough ballpark estimate of the cost, two trials would be $23 million USD.
Formula is a big deal for retinoids because of irritation – it’s the main reason people stop using them. There are lots of hacks for making retinoids less irritating (there’s a guide from me here). But almost everyone who uses retinoids will at some point accidentally apply too much, and end up red, itchy, peeling and stinging (unless you’re genetically blessed – there does seem to be a big genetic component to it).
Related post: How to Start on Tretinoin (Retin-A) and Retinol
Why irritation happens with retinoids isn’t 100% clear. It’s partly because of how retinoids work – activating retinoid receptors leads to faster production of epidermal cells, which results in peeling and a less mature skin barrier. There’s also increased inflammatory cytokines, mast cell activation, and activating pain receptors.
Related post: Is Retinol a Scam? The Science
A lot of these aspects could be counteracted by changing the formulation: adding anti-irritant skincare ingredients, strategies to slow down or even out the delivery of the active into the skin (e.g. encapsulation, polymers).
- A 0.025% tretinoin gel (Avita) containing polyolprepolymer-2 caused less dryness and peeling than the standard 0.025% tretinoin gel (Retin A).
- Some studies indicate that cream bases are less irritating
- Far fewer people reported side effects in the clinical trials for Altreno, with its fancy lotion base, compared to the equivalent gel formula which contained similar anti-irritant ingredients (collagen, glycerin, hyaluronic acid):
| Side effect | 0.05% Tretinoin Gel (Atralin) | 0.05% Tretinoin Lotion (Altreno) |
|---|---|---|
| Dryness | 16% | 4% |
| Peeling/exfoliation | 12% | 1% |
| Stinging/burning/pain | 8–9% | 3% |
| Redness (erythema) | 7% | 2% |
These anti-irritation formulation features show up a lot in cosmetic retinoid formulas, but not in drug formulas, which tend to be very basic.
This lack of flexibility in formula is also annoying if your skin is sensitive to a particular inactive ingredient. There’s also a lot less options when it comes to percentages, or combinations with other active ingredients, or even just cosmetic elegance – a lot of drug creams and gels are just really basic, generic formulas that haven’t changed in decades (and feel that way too).
Buffering
Anecdotally, there’s a lot less leeway when it comes to accidentally applying too much of a drug retinoid compared to cosmetic retinoids, which seem to have a lot more room for error in terms of side effects (peeling, irritation, stinging etc.).
This might be because of how cosmetic retinoids are converted in skin. Cosmetic retinoids are mostly ingredients that need to be converted into tretinoin to work properly. This is often viewed as being purely a downside, making them weaker and less likely to work. But on the irritation front, this can be an upside – essentially, it means cosmetic retinoids have the potential to essentially act as self-limiting, time-release versions of tretinoin.
The conversion from a retinyl ester to tretinoin takes place over 3 steps:
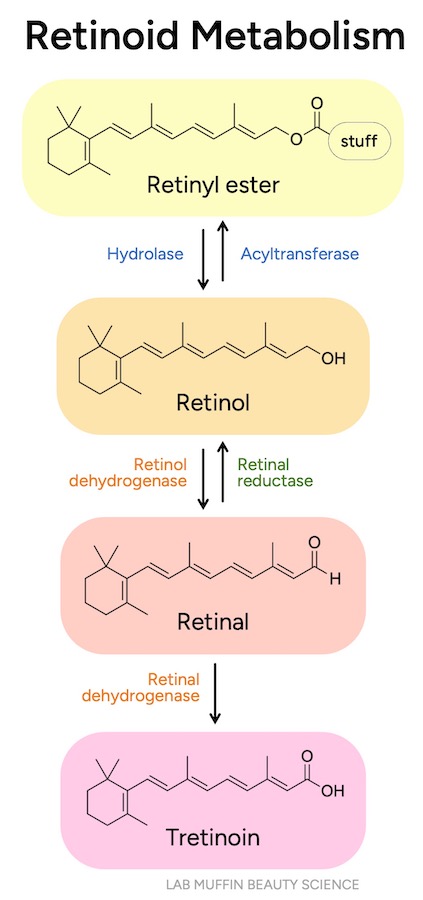
Steps 1 and 2 are reversible, which is the self-limiting part. If you’ve done some chemistry, you’ll know the concept of equilibrium, and how this works as a buffer – it’s a similar concept. Essentially, there’s an extra system in place for buffering retinyl esters, retinol and retinal. If you’ve applied too much of any of these, it can kind of overflow and turn into some of the other things. But because the conversion to tretinoin is irreversible (there’s no arrow going back), there’s a lot less leeway if you apply tretinoin.
Availability
The other big advantage with cosmetic retinoids (most of the time) is availability. For prescription products, you obviously need to be eligible for a script and get it through a doctor, unlike cosmetics which have less barriers.
There’s also the problem with limited drug formulas and manufacturers. Some countries don’t have particular options approved (you can’t get tazarotene easily in Australia, for example). Sometimes an option will be discontinued and you won’t have a good alternative. Because there are less barriers when it comes to launching new non-drug products on the market, this is less of an issue for cosmetic retinoids.
Drug or cosmetic?
So, should you go for drug or cosmetic retinoids? Before we start – I’m a chemist, not a medical doctor, and I don’t know all the specifics of your situation. So these are general guidelines, and you should book a consult with a dermatologist who can assess your skin and individual situation if you’re not sure.
Strength and tolerance
Drug retinoids are generally stronger than cosmetic retinoid products, and they aren’t formulated to reduce irritation that much, so most people have to use them really carefully at the start – I have a guide on how to do that – but most people still end up having some irritation. So think about:
- Can your skin handle retinoids?
This is not necessarily the same as how well your skin handles other irritating ingredients. I’m a prime example – my skin is really tolerant of hydroxy acids, so I thought I’d be fine with retinol. I was not, my skin leapt off my face.
If you’ve used retinoids before and your skin can tolerate them, drug retinoids might be a better option. But if you haven’t used them before, I’d recommend a cosmetic retinoid as your first product. There does also seem to be a genetic component to retinoid irritation, so if you have relatives you can ask, that could help. In studies, East Asians seem to be less tolerant of retinoids. Irritation is also a bigger issue for melanin-competent skin, since post-inflammatory hyperpigmentation is more of a concern, and it’s usually one of the reasons for using retinoids in the first place.
- Is your skin sensitive in general?
Retinoids have a bunch of side effects that are pretty inherent to how they work, and a lot of them involve having a more impaired barrier, at least temporarily. People with more sensitive skin tend to be less tolerant of retinoids. If your barrier isn’t great at the best of times it’s probably best to start with a gentler cosmetic retinoid.
Availability and Price
- Which products are available where you are?
- Which one has affordable options?
This depends on where you are and your budget.
For drugs, there are more limited options. Different brands are different prices, and some drug ingredients come in generic versions that are more affordable.
It also depends on the pack size – in Australia we had this really cheap generic tretinoin cream that was $25 for 30 mL that got discontinued, we still have one that’s a decent price per mL but it’s in a larger tube, so there’s a higher upfront cost.
And for prescription retinoids, you’ll also have to factor in the cost of the doctor’s appointment, assuming the doctor agrees that retinoids are a good idea for you, and you might need to be referred to a dermatologist in some places.
Online overseas pharmacies
You can also import prescription retinoids online from overseas pharmacies usually at a low price, and a lot of them aren’t super fussy about whether you have a script – some people like this option but I’m not a huge fan.
When you import from overseas, a lot of the time you end up being covered by neither country’s regulations (domestic drug regulation and export is usually different), which again just cancels out a lot of the advantages of drug retinoids being regulated: the guaranteed efficacy, stability, quality control. If you do go down this route, make sure you thoroughly vet reviews online for things like the quality of the product and whether the store is known for credit card scams.
Compounded drug retinoids
There is a kind of middle route, which are compounded drug retinoids.
Compounding is when a specially trained pharmacist mixes up a custom formula from the prescribing doctor – for example, a cream with 0.05% tretinoin, 5% azelaic acid and 4% niacinamide. This might sound like you’re getting the best of both worlds – you’re getting a custom formula with exactly the actives you want, at effective concentrations! But if you think about all the pros and cons from before, you actually lose a lot of the advantages of drug AND cosmetic retinoids.

Yes, you get the more effective drug retinoid as the active ingredient. But because it’s custom, the formula isn’t tested for efficacy or stability. Compounding pharmacists will look for obvious clashes, then mix the ingredients into a generic base (there are a few different bases used), but they’re not going to run a clinical trial or a stability test on your custom formula. So for something unstable or a bit difficult to get into skin, the efficacy and stability will almost definitely end up worse than for off-the-shelf drug formulas, and even cosmetic skincare products that have been properly tested.
Formula flexibility also isn’t as great as you’d expect. You do get to combine some active ingredients, but you only get to choose out of the ones that compounding pharmacy has (if you get a choice at all – depends on your prescribing doctor). There’s probably only one base available, and the cosmetic elegance of standard compounding bases is usually… not great. They’re usually really basic medical creams designed to be compatible with a wide range of different drug actives, not for a pleasant user experience.
There are some telederm “prescription skincare” services that specialise in compounded tretinoin, like Apostrophe, Curology, Hers, Dermatica and Software. These services tend to use their own special bases.
Because these companies only really prescribe a limited number of formulas, they could in theory try to optimise their most popular combinations for stability and efficacy. But I haven’t seen much to suggest that any of them do that – usually their expiry dates are the standard compounding 3-4 months (versus an off-the-shelf drug retinoid or a cosmetic retinoid from a good brand, which usually lasts 6-12 months after opening).
Their special bases do tend to feel a bit nicer than the generic compounding ones, but that isn’t a guarantee either. Pretty much every brand has reviews saying their newly opened product has scratchy crystals in it, which is a pretty basic stability issue that would’ve been picked up for the vast majority of cosmetic products.
Honestly, I think a better option for most people would be layering an off-the-shelf drug retinoid with a cosmetic skincare product with the other ingredients you want. It’s less convenient for application (two products instead of one), but you get good stability for the separate products. There’s also some degree of efficacy testing (for the drug, and perhaps the cosmetic product if you choose carefully). You might compromise it a bit if you mix them, but it’s likely better than no testing, and you can leave some time in between the layers to try to make each layer as close to testing as possible.
But it still depends on your specific situation – it can work out to be a good option for some people if the telederm process is really smooth, and it can end up really cost-effective.
So those are your options – remember you don’t have to choose only drug or only cosmetic retinoids – I personally use a mix depending on how robust my skin is feeling.
Next time we’ll talk about the differences between the drug retinoids, then move into the murky waters of cosmetic retinoids.
(Thanks to my ex-student Sam, a pharmacist and pharmacy instructor, for helping me out with the details of compounding, and thanks to Ruby for feedback on the outline!)
References
Good general references on retinoids:
- Baumann LS. Retinoids. In: Baumann LS, Rieder EA, Sun MD, eds. Baumann’s Cosmetic Dermatology. 3rd ed.; McGraw Hill; 2022:615-630.
- Sorg O, Kaya G, Saurat JH. Topical Cosmeceutical Retinoids. In: Draelos ZD, ed. Cosmetic Dermatology: Products and Procedures. 3rd ed.; John Wiley & Sons; 2023:408-419.
Rendon M, Berneburg M, Arellano I, Picardo M. Treatment of melasma. J Am Acad Dermatol. 2006;54(5 Suppl 2):S272-S281. doi:10.1016/j.jaad.2005.12.039
US Food and Drug Administration (FDA). The FDA’s Drug Review Process: Ensuring Drugs Are Safe and Effective. Published November 27, 2017. Accessed November 23, 2023.
US Food and Drug Administration (FDA). Development & Approval Process. Published August 8, 2022. Accessed November 23, 2023.
Therapeutic Goods Administration (TGA). How we regulate medicines. Published June 20, 2019. Accessed November 23, 2023.
US Food and Drug Administration (FDA). Draft guidance on tretinoin (topical gel). October 2022.
US Food and Drug Administration (FDA). Draft guidance on tretinoin (topical cream). February 2019.
International Conference on Harmonisation (ICH). Stability Testing of New Drug Substances and Products Q1A(R2). February 2003.
US Food and Drug Administration (FDA). Expiration Dates – Questions and Answers. Published October 24, 2022. Accessed November 23, 2023.
Therapeutic Goods Administration (TGA). Australian regulatory guidelines for OTC medicines, Appendix 2 Section 9. Stability of the finished product. July 2021.
Temova Rakuša Ž, Škufca P, Kristl A, Roškar R. Retinoid stability and degradation kinetics in commercial cosmetic products. J Cosmet Dermatol. 2021;20(7):2350-2358. doi:10.1111/jocd.13852
US Food and Drug Administration (FDA). CFR—Code of Federal Regulations, Title 21, Part 211 – Current Good Manufacturing Practice for Finished Pharmaceuticals. Accessed November 23, 2023.
US Food and Drug Administration (FDA). Facts About the Current Good Manufacturing Practices (CGMP). Published May 31, 2023. Accessed November 23, 2023.
Therapeutic Goods Administration (TGA). Good manufacturing practice – an overview. Published June 21, 2022. Accessed November 23, 2023.
European Commission. Safety Gate Alert Number: A11/00065/22. Published May 20, 2022. Accessed November 23, 2023.
Hubinger JC. Determination of retinol, retinyl palmitate, and retinoic acid in consumer cosmetic products. J Cosmet Sci. 2009;60(5):485-500. doi:10.1111/j.1468-2494.2010.00578_2.x
Temova Rakuša Ž, Škufca P, Kristl A, Roškar R. Quality control of retinoids in commercial cosmetic products. J Cosmet Dermatol. 2021;20(4):1166-1175. doi:10.1111/jocd.13686
Gupta R, Morten CJ, Zhu AY, Ramachandran R, Shah ND, Ross JS. Approvals and Timing of New Formulations of Novel Drugs Approved by the US Food and Drug Administration Between 1995 and 2010 and Followed Through 2021. JAMA Health Forum. 2022;3(5):e221096. doi:10.1001/jamahealthforum.2022.1096
Center for Drug Evaluation and Research. Multi-disciplinary Review and Evaluation NDA 209353. February 1, 2016.
Sertkaya A, Wong HH, Jessup A, Beleche T. Key cost drivers of pharmaceutical clinical trials in the United States. Clin Trials. 2016;13(2):117-126. doi:10.1177/1740774515625964
Macgregor JL, Maibach HI. Specificity of Retinoid-Induced Irritation and Its Role in Clinical Efficacy. In: Zhai H, Wilhelm KP, Maibach HI, eds. Dermatotoxicology. 7th ed. CRC Press; 2008:423-430. (The earlier version of this article is doi:10.1159/000058335)
Varani J, Fligiel H, Zhang J, et al. Separation of retinoid-induced epidermal and dermal thickening from skin irritation. Arch Dermatol Res. 2003;295(6):255-262. doi:10.1007/s00403-003-0416-5
Jacobson MK, Kim H, Coyle WR, et al. Effect of myristyl nicotinate on retinoic acid therapy for facial photodamage. Exp Dermatol. 2007;16(11):927-935. doi:10.1111/j.1600-0625.2007.00616.x
Kim B, Kim JE, Kim H, Lee JD, Choi KY, Lee SH. Co-treatment with retinyl retinoate and a PPARα agonist reduces retinoid dermatitis. Int J Dermatol. 2012;51(6):733-741. doi:10.1111/j.1365-4632.2011.05332.x
Del Rosso J, Sugarman J, Green L, et al. Efficacy and safety of microencapsulated benzoyl peroxide and microencapsulated tretinoin for the treatment of acne vulgaris: Results from two phase 3 double-blind, randomized, vehicle-controlled studies. J Am Acad Dermatol. 2023;89(4):719-727. doi:10.1016/j.jaad.2023.05.093
Lucky AW, Cullen SI, Jarratt MT, Quigley JW. Comparative efficacy and safety of two 0.025% tretinoin gels: results from a multicenter double-blind, parallel study. J Am Acad Dermatol. 1998;38(4):S17-S23. doi:10.1016/s0190-9622(98)70141-0
Dosik JS, Homer K, Arsonnaud S. Cumulative irritation potential of adapalene 0.1% cream and gel compared with tretinoin microsphere 0.04% and 0.1%. Cutis. 2005;75(4):238-243.
Culp L, Moradi Tuchayi S, Alinia H, Feldman SR. Tolerability of Topical Retinoids: Are There Clinically Meaningful Differences Among Topical Retinoids?. J Cutan Med Surg. 2015;19(6):530-538. doi:10.1177/1203475415591117
Veraldi S, Barbareschi M, Benardon S, Schianchi R. Short contact therapy of acne with tretinoin. J Dermatolog Treat. 2013;24(5):374-376. doi:10.3109/09546634.2012.751085
Zheng Y, Che D, Peng B, et al. All-trans-retinoic acid activated mast cells via Mas-related G-protein-coupled receptor-X2 in retinoid dermatitis. Contact Dermatitis. 2019;81(3):184-193. doi:10.1111/cod.13292
Yin S, Luo J, Qian A, et al. Retinoids activate the irritant receptor TRPV1 and produce sensory hypersensitivity. J Clin Invest. 2013;123(9):3941-3951. doi:10.1172/JCI66413
Kedishvili NY. Enzymology of retinoic acid biosynthesis and degradation. J Lipid Res. 2013;54(7):1744-1760. doi:10.1194/jlr.R037028
Leyden J, Grove G, Zerweck C. Facial tolerability of topical retinoid therapy. J Drugs Dermatol. 2004;3(6):641-651.
Callender VD, Baldwin H, Cook-Bolden FE, Alexis AF, Stein Gold L, Guenin E. Effects of Topical Retinoids on Acne and Post-inflammatory Hyperpigmentation in Patients with Skin of Color: A Clinical Review and Implications for Practice. Am J Clin Dermatol. 2022;23(1):69-81. doi:10.1007/s40257-021-00643-2
Kikuchi K, Suetake T, Kumasaka N, Tagami H. Improvement of photoaged facial skin in middle-aged Japanese females by topical retinol (vitamin A alcohol): a vehicle-controlled, double-blind study. J Dermatolog Treat. 2009;20(5):276-281. doi:10.1080/09546630902973987
Tadaki T, Watanabe M, Kumasaka K, et al. The effect of topical tretinoin on the photodamaged skin of the Japanese. Tohoku J Exp Med. 1993;169(2):131-139. doi:10.1620/tjem.169.131
Samantha L (pharmacist), Personal Communication. September 13, 2023.





so informative! do you have any OTC recommendations that has tretinoin? thank you!
In the US there is a telemedicine site which does Altreno and brand-name original Retin-A. They charge $20 for the consult and the mail-order cash price is $40 for 45g original Retin-A and $115 for 45g of Altreno. Generic tretinoin is $30-$50, but you need to pay a fee to the physician. If you are older nd on public Medicare, they might not take insurance for the visit. You need a coupon code to go to a pharmacy to get Altreno $115 (vs $160) if you are not going through insurance. And if it’s not for acne, you are paying cash anyway.
You mentioned the importance of the base formulation. Altreno’s studies showed that it was more effective than the lotion base for treating acne, but actually the lotion base seemed to be effective too! (51% vs 40%) Maybe this was a benefit for teenager boys who don’t moisturize.